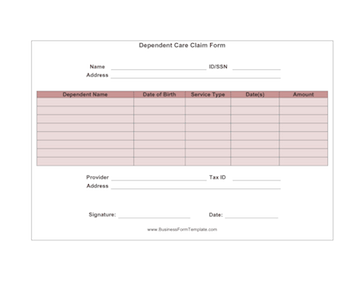
Dependent Care Claim Form
Use this form to fill in the information when you need to be reimbursed for services provided for your dependent.
Downloads are subject to this site's terms of use.
Description
Dependent Care Claim Form
Fields: name, address, dependent name, date of birth, service type, date(s), amount, provider, address, tax ID, signature