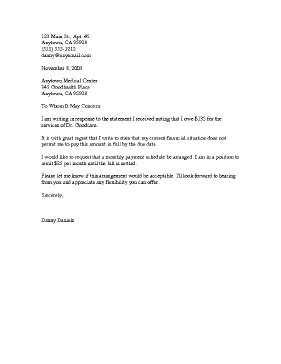
Request Medical Payment Plan
This letter, intended to be customized in Microsoft Word, is to be used when seeking a payment plan for medical bills.
Downloaded > 4,000 times
Downloads are subject to this site's terms of use.
Description
123 Main St., Apt. #5
Anytown, CA 95928
(555) 555-1212
[email protected]
November 8, 2008
Anytown Medical Center
345 Goodhealth Place
Anytown, CA 95928
To Whom It May Concern:
I am writing in response to the statement I received noting that I owe $135 for the services of Dr. Goodcare.
It is with great regret that I write to state that my current financial situation does not permit me to pay this amount in full by the due date.
I would like to request that a monthly payment schedule be arranged. I am in a position to remit $25 per month until the bill is settled.
Please let me know if this arrangement would be acceptable. I'll look forward to hearing from you and appreciate any flexibility you can offer.
Sincerely,
Danny Daniels